Dry eye is one of the most common eye problems and affects millions of people. However, the symptoms of dry eye are often misunderstood and under-treated.
Many people with dry eye do not think that their eyes feel dry – often they are complaining of too much tearing or watery eyes. Another common symptom of dry eye is blurry vision with computer use, or towards the end of the day – people often feel that they have to blink or “refocus” their vision. Other common issues are a dull ache or pain in the eye or behind the eye, a foreign body feeling, like there is sand, or an eyelash in the eye, or sensitivity to light. Other people find that they cannot tolerate their contact lenses, especially towards the end of the day.
Dry eye is a bad name for this condition. In fact, this condition is very poorly named – as for most people – it is neither a “dry” problem” or an “eye” problem. In most people, dry eye is a problem with the oil glands of the eyelids.
(This condition has many names and can also be called aqueous tear deficiency, blepharitis, keratitis sicca, meibomian gland dysfunction, or ocular rosacea.) The best name for this condition is dysfunctional tear syndrome – because the functional problem is that the tear film quality is very poor – but these multiple names usually refer to the same underlying problem.
Dysfunctional tear syndrome has 2 major types. In people under 30, or people with systemic conditions such as Rheumatoid Arthritis, Lupus, Sjogren’s syndrome, and from certain medications, the cause of the problem is often due to a decreased production of the watery tears from the lacrimal glands, which sit on top of the eye. This is sometimes called aqueous tear deficiency.
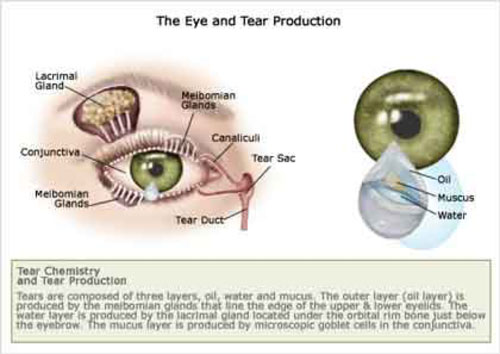
The most common type of dysfunctional tear syndrome is called meibomian gland dysfunction (MGD) or ocular rosacea, and is due to a lack of production of the oily tears, called meibum, produced in the meibomian glands. (Just as we have saliva in our mouths made from the salivary glands, and oils on our skin and hair called seibum from the sebaceous glands, we have meibum produced from the meibomian glands in the eye lids – the hardened meibum is the crust-like discharge that we often remove from our eyes upon awakening) MGD is more common in people over 40, people with light color skin, blue or green colored eyes, and hair, and people with rosacea.
As a lack of seibum (skin oils) causes dry skin and hair, a dysfunction of meibum causes dysfunction of the tear film. When the sebaceous glands of the skin get blocked, this causes pimples. Similarly, when the meibum cannot flow, the oils get “backed up” and this causes styes, also called a chalazion, and causes the symptoms of “dry eye”.
We need the oils produced in the meibomian glands to coat the surface of the eye, and these oils keep the natural aqueous or watery tears on the eye. When the meibomian oils are not present, the natural watery tears do not stay on the eye. For this reason, people with MGD often complain about too much tearing or watery eyes. The eye keeps trying to replace the watery tears that should have been covered by the oily tears. (Just as licking chapped lips does not help, the body cannot “fix” this problem by making more watery tears. This is also why over-the-counter tears do not help. As we need chapstick or Vaseline to heal chapped lips, we need functional oils from the meibomian glands or oily tears, such as Oasis plus, Systane Balance and Refresh Optive Advanced Preservative Free.
Sometimes people have a combination of aqueous tear deficiency and MGD. Knowing the type of dysfunctional tear film allows us to choose the proper therapy.
Many people mistakenly think that dry eye is a minor problem, and they shouldn’t bother their doctor with these issues. Other people see their eye doctor with dry eye symptoms and they are told that it is “just dry eye” and to use over the counter tear drops and not to worry about it.
We often see patients who tell us that they are being treated for pink eye, or that they get frequent “eye infections” and have been treated with antibiotics by their internist, or at an urgent care center. They are told that they have “pink eye” or “conjunctivitis” due to the redness of the eyes and a yellow discharge, often worse in the morning. In fact, bacterial infection of the conjunctiva is quite rare – we see only a few cases per year and “pink eye” is caused by virus, and has no known treatment. While some people feel better after receiving antibiotic eye drops, this is usually due to the lubricating effect of the eye drops, and often the antibiotics are combined with a steroids, which treats the true underlying problem, a dysfunctional tear film. Viral conjunctivitis has no known treatment, starts in one eye, and the affected eye gets VERY red, and then the other eye is affected in 3-4 days, and then both eyes are red for 10-14 days. If you have had “pink eye” and you felt better in a few days after using eye drops, then you did not have a viral infection. Also, viral conjunctivitis is very contagious and your close contacts will develop the same problem after the incubation period of two weeks. Just as it is rare to have frequent bouts of the “flu”, it is uncommon to have frequent bouts of “pink eye” and the vast majority of people with this history have meibomian gland dysfunction.
At our office, we realize that dry eye is a serious condition and can often decrease one’s quality of life. We take a full medical history, including your medications, and any past dry eye treatments. We aim to aggressively treat dry eye problems using medications including steroid eye drops, Restasis, Xiidra, punctal plugs, Omega 3 fatty acid supplements, and Doxycycline or Minocycline.
However, we see many patients who have used the above treatment for months or years without relief. This is because these therapies often do not address the main problem, the blocked meibomian glands. Just as putting the best fuel in the gas tank of your car will not help if the fuel injectors are blocked, when the meibomian glands are blocked, the symptoms of dysfunctional tear syndrome will not resolve. We have access to the latest treatments in dry eye therapy, aimed at improving the oily tears made in the meibomian glands.
Our most successful treatment is intense pulsed light (IPL) for meibomian gland dysfunction. IPL is used mostly by dermatologists to treat rosacea of the face. We now realize that MGD is more of a dermatologic problem than a primary ocular problem. The IPL heats and melts the blocked oils and then these oils are expressed, and released. The IPL also causes regression of the redness of the eyelids and face, and many people like the cosmetic improvement in their facial skin.
We find that our patients find significant relief after 1 to 2 treatments. Some people will need the treatment repeated every 4-6 months (Just as we need our teeth cleaned every 6 months, we have found that some people have the best results when they repeat the IPL treatments every 4-6 months)
We are also one of the only eye doctors in Baltimore to have access to Lipiflow. Lipiflow is a novel technology which uses warmth and gentle pressure to open the blocked meibomian glands and often resolves dry eye symptoms shortly after one treatment.
Blephex is also an option for treating MGD. Dr. Levinson can be seen discussing this technique on WBAL with Donna Hamilton (link to Dr. Levinson presents Blephex) and you can watch an animation about Blephex.
In fact, Dr. Levinson also suffers from meibomian gland dysfunction and has had multiple IPL and Lipiflow treatments himself.
We also offer Meibomian gland probing, which opens the blocked oil glands and allows tears to flow more naturally. See the video describing this technique.
We also offer treatment of dry eyes with Amniotic membrane. This technique uses the healing properties and anti-inflammatory nature of amniotic membrane, to make the eyes feel better.
In conjunction with Hunt Valley Compounding pharmacy, we also offer autologous serum tears (NovoTears). Some patients have had significant improvement in their symptoms with this treatment.
Please feel free to call our office with any questions about dry eye therapy, and to make an appointment with Dr. Levinson for an evaluation.
